
When you pick up a prescription, you might not think twice about whether it’s the brand-name drug or the cheaper generic. But behind that simple swap is a powerful system designed to keep you safe - therapeutic equivalence. It’s not just marketing. It’s science. And it’s the reason millions of Americans can switch to generics without risking their health.
What therapeutic equivalence actually means
Therapeutic equivalence isn’t just about two pills looking similar or having the same active ingredient. It means they work the same way in your body - the same speed, the same strength, the same safety profile. The U.S. Food and Drug Administration (FDA) defines it clearly: two drugs are therapeutically equivalent if they contain the same active ingredient, in the same dose, form, and route, and they’ve been proven to deliver the same clinical results. That’s it. No guesswork. No assumptions.This isn’t a suggestion. It’s a legal standard. The FDA uses its Orange Book - officially called the Approved Drug Products with Therapeutic Equivalence Evaluations - to list every drug that meets this bar. As of October 2023, over 13,000 drug products are listed there. Each one has a two-letter code: A means it’s approved as interchangeable. B means it’s not. If your generic has an AB rating, you can trust it.
How the FDA proves drugs are truly equivalent
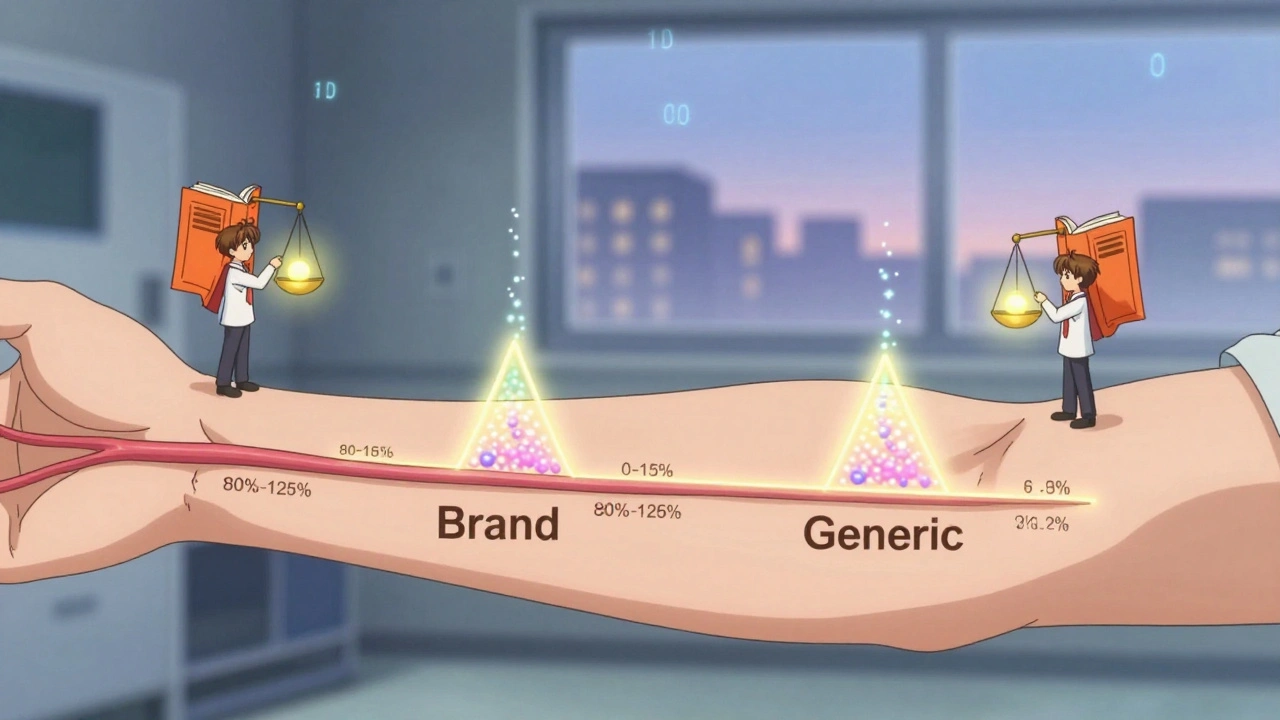
The FDA doesn’t just look at the label. They test how your body absorbs the drug. That’s called bioequivalence. For a generic to be approved, its absorption rate and total amount absorbed must fall within 80% to 125% of the brand-name drug. That’s not random. It’s based on decades of data showing this range doesn’t affect clinical outcomes for most people.Here’s how it works: volunteers take both the brand and the generic. Blood samples are taken over time to measure how much of the drug enters the bloodstream (AUC) and how fast it peaks (Cmax). If the 90% confidence interval for those numbers stays between 80% and 125%, the drugs are bioequivalent. That’s the gold standard. For most drugs, that’s enough.
But not all drugs are the same. For drugs with a narrow therapeutic index - like warfarin, levothyroxine, or lithium - even small differences can matter. That’s why the FDA requires tighter limits for these: 90% to 110%. These drugs are flagged in the Orange Book. Pharmacists and doctors know to be extra careful.
Why therapeutic equivalence beats therapeutic interchange
Some people confuse therapeutic equivalence with therapeutic interchange. They’re not the same. Therapeutic interchange means swapping one drug for another in the same class - like switching from one statin to another. That’s not based on identical chemistry. It’s based on similar effect. And that’s riskier.A 2019 study in JAMA Internal Medicine found that therapeutic interchange led to 32% more adverse events than switching to a therapeutically equivalent generic. Why? Because different drugs, even in the same class, can have different side effects, interactions, or absorption patterns. Therapeutic equivalence avoids that entirely. You’re not guessing. You’re replacing one exact version with another.
Real-world safety data: Are generics really safe?
Some patients worry: “What if my body reacts differently to the generic?” That’s understandable. But the data says otherwise. A 2022 survey of 12,500 UnitedHealthcare patients found that 87% reported no change in how their medication worked after switching to an FDA-approved generic. Only 3.2% blamed the switch for any side effects.When you dig deeper into the rare cases where people report problems, most don’t involve true therapeutic equivalence. The Institute for Safe Medication Practices reviewed 127 adverse event reports between 2018 and 2022. Only 17 involved drugs with an AB rating. The rest were either non-equivalent products, mislabeled generics, or cases where anxiety about the switch caused perceived side effects.
One Reddit thread from 2021 had 47 reports of issues after switching. Only 3 of those involved an AB-rated drug. The rest were either B-rated products or cases where a different drug was substituted entirely - not a true generic.
What pharmacists and doctors need to know
Pharmacists are on the front lines. In 49 states, they can automatically substitute a therapeutically equivalent generic unless the prescriber says “dispense as written.” That’s because the system works. But they have to know how to read the Orange Book. The two-letter code isn’t just jargon - it’s a safety tool.The first letter tells you if it’s equivalent (A) or not (B). The second letter gives extra info - like whether it’s an extended-release version or if it’s a complex product. Doctors need to understand this too. If you write a prescription for “lisinopril,” you’re not specifying a brand. That’s fine - because the system assumes therapeutic equivalence. But if you’re prescribing a drug like levothyroxine, you might want to specify the brand or ask for the generic with the exact formulation your patient has been stable on.
The FDA offers free online training for healthcare providers. After a 90-minute course, 85% of participants improved their ability to correctly identify therapeutic equivalence. That’s not just helpful - it’s essential.
When therapeutic equivalence doesn’t apply
Not all drugs can be easily tested for bioequivalence. Inhalers, topical creams, eye drops, and some injectables have complex delivery systems. The active ingredient might be the same, but how it gets into your body can vary. The FDA acknowledges this. For these products, they’re developing new methods - like using advanced imaging or clinical endpoint studies instead of just blood levels.In 2023, the FDA released draft guidance for topical corticosteroids, recognizing that traditional bioequivalence tests aren’t enough. They’re also investing $65 million through GDUFA III to improve testing for complex generics through 2027. And they’re working with MIT on AI models to predict which formulation changes might affect outcomes - before they even hit the market.
The economic impact - and why it matters for you
Therapeutic equivalence saves money. A lot of it. Since 2009, generic drugs have saved the U.S. healthcare system $1.7 trillion. In 2022 alone, they saved $158 billion. That’s not just corporate profit. That’s lower copays. Fewer skipped doses. More people getting the meds they need.Today, 90.7% of all prescriptions filled in the U.S. are generics. Yet they make up only 58% of total drug spending. That’s the power of therapeutic equivalence - it lets you get the same treatment for a fraction of the cost.
And when brand-name drugs go on shortage - which happens often - therapeutic equivalence is what keeps treatment going. About 78% of switches to generics occur during shortages. Without this system, patients would face delays, higher prices, or worse outcomes.
What’s next for therapeutic equivalence
The system isn’t perfect. But it’s evolving. As more complex drugs - like biosimilars - enter the market, the FDA is building new frameworks. Biosimilars aren’t classified under therapeutic equivalence. They have their own “interchangeability” designation, which requires even more data.But the core principle stays the same: if a drug is supposed to do the same thing as another, it should act the same way. That’s patient safety. That’s science. That’s therapeutic equivalence.
Are generic drugs really as safe as brand-name drugs?
Yes, if they’re rated as therapeutically equivalent (AB) by the FDA. The FDA requires generics to match brand-name drugs in active ingredient, strength, dosage form, and how the body absorbs them. Over 90% of prescriptions in the U.S. are generics, and studies show they work the same way with the same safety profile. Rare reports of issues usually involve non-equivalent products or patient anxiety, not actual differences in drug performance.
What does the AB rating mean on my prescription?
The AB rating comes from the FDA’s Orange Book. The first letter, A, means the drug is therapeutically equivalent to the brand-name version. The second letter, B, means it’s not. If your generic has an AB rating, you can safely switch without worrying about changes in effectiveness or side effects. Always check the label or ask your pharmacist if you’re unsure.
Can I always switch to a generic without talking to my doctor?
In most cases, yes - but not always. Forty-nine states allow pharmacists to substitute therapeutically equivalent generics automatically. However, for drugs with a narrow therapeutic index - like warfarin or levothyroxine - your doctor may write “dispense as written” to prevent switching. If you’ve been stable on a specific brand or generic, it’s smart to ask before changing.
Why do some people say generics don’t work for them?
Sometimes, it’s not the drug - it’s the switch. Changing from one pill to another, even if it’s identical, can cause anxiety or minor side effects from new fillers or coatings. In rare cases, patients are switched to a non-equivalent product (B-rated) or a different drug entirely. If you notice changes after switching, talk to your pharmacist. Check the Orange Book rating. Most issues aren’t due to the active ingredient - they’re about perception or error.
Are there drugs that can’t be made as generics?
Yes. Some complex products - like inhalers, certain creams, and injectables - are hard to copy exactly because their delivery systems matter as much as the drug itself. The FDA has special rules for these, and they’re still developing better testing methods. For now, many of these drugs don’t have approved generics. Biosimilars are a separate category altogether and require different approval standards.
What you can do to stay safe
- Always check the drug name on your prescription and the label. If it’s a generic, look for the AB rating. You can search the FDA’s Orange Book online for free. - If you’re on a narrow therapeutic index drug, ask your doctor if you should stick with one brand or generic. - Don’t assume all generics are the same. If you switch and feel different, speak up. It’s not just in your head - it’s worth investigating. - Use your pharmacist as a resource. They’re trained to spot therapeutic equivalence and can explain what’s in your medication.Therapeutic equivalence isn’t just a regulatory box to check. It’s the quiet guarantee that you can afford your medicine without sacrificing your health. And that’s worth understanding.
amit kuamr
Generic drugs work fine for most people but dont act like the FDA is some infallible god. I seen too many cases where generics caused weird side effects that brand never did. Bioequivalence my ass. Bodies arent lab rats.
elizabeth muzichuk
Ugh. Another one of those 'trust the system' lectures. I switched to a generic lisinopril and got dizzy for two weeks. My doctor said it was 'just anxiety' but I know better. The FDA doesn't test for how you FEEL. Only how much drug is in your blood. That's not safety, that's bureaucracy pretending to care.
Karandeep Singh
AB rating? More like A for assumed B for bullshit. Why do they even have a second letter if its just noise?
Debbie Naquin
Therapeutic equivalence is a statistical abstraction that assumes homogeneity in human pharmacokinetics. But we're not Gaussian distributions. We're messy biological systems with epigenetic variations, gut microbiome differences, and metabolic polymorphisms that render the 80-125% window dangerously reductive. The FDA's model is elegant but ontologically naive.
Mary Ngo
Have you ever considered that the FDA is influenced by Big Pharma? The Orange Book is a carefully curated illusion. They approve generics that are 'close enough' so the big companies can keep their patents and profits. That 90.7% generic rate? It's not because they're safe-it's because they're cheaper to force on us.
James Allen
Look, I love America. And America makes the best drugs. When I see some cheap generic from India or China with an AB rating, I just shake my head. We built this system to protect people-not let them swallow mystery pills from overseas factories. I don't care how many studies say it's fine. I trust American-made medicine. Period.
Alexander Williams
The 80-125% bioequivalence window is mathematically valid for population-level outcomes but ignores individual pharmacodynamic variance. For drugs with nonlinear kinetics or transporter saturation-like phenytoin or cyclosporine-this range is clinically meaningless. The FDA’s framework is a relic of 1980s regulatory pragmatism, not modern pharmacology.
Suzanne Mollaneda Padin
As a pharmacist for 18 years, I’ve seen patients panic over generics. Most of the time, it’s the coating or filler causing stomach upset-not the active ingredient. I always check the Orange Book, explain the AB rating, and remind them: if they feel off, we can switch back. No shame in that. Safety isn’t just about chemistry-it’s about trust.
Amber-Lynn Quinata
AB rating? 😔 I switched to a generic levothyroxine and my TSH went from 2.1 to 8.9. My doctor said it was 'just coincidence.' Coincidence? I’ve been stable on Synthroid for 10 years. Now I’m on a waiting list for a brand because my insurance won't cover it. This system is rigged. 💔
Lauryn Smith
I get why people are nervous. Switching meds is scary. But if you’re worried, talk to your pharmacist. They can tell you if it’s AB-rated and even help you get the brand if needed. You’re not alone in this. And you deserve to feel safe with your meds. No one should have to guess.
Bonnie Youn
GENERIC DRUGS SAVE LIVES AND MONEY 💪 You think you’re being brave by refusing them? Nah-you’re just making healthcare unaffordable for everyone else. Millions rely on generics to even get their meds. Stop letting fear drive your choices. The science is solid. Trust the process. You got this! 🙌
Charlotte Collins
Let’s not pretend this is about safety. It’s about cost-shifting. The FDA’s 'equivalence' standards are designed to minimize litigation risk, not optimize outcomes. And when patients report adverse events? They get labeled as 'anxiety' or 'perception.' The system doesn’t want to admit it’s flawed-it just wants the paperwork to look clean.